
This theory is likely the easiest to get your head around and provides an exceptional amount of information about how the human body moves, and what happens when there is a breakdown in the chain. ‘The chain’ is just another way to refer to the body in terms of movement; encompassing the notion that the body does not move segmentally but rather that our segments work together to create global movement. It also acknowledges that any change to one segment will affect other areas of ‘the chain.’
Broken down, the theory looks at each joint’s individual role in the body which can usually be categorized into mobilization or stability. This is largely dictated by the anatomical make up of each joint.
Mobility: the ability to access the required range of motion for the function of a specific joint
Stability: the ability to resist internal and external forces
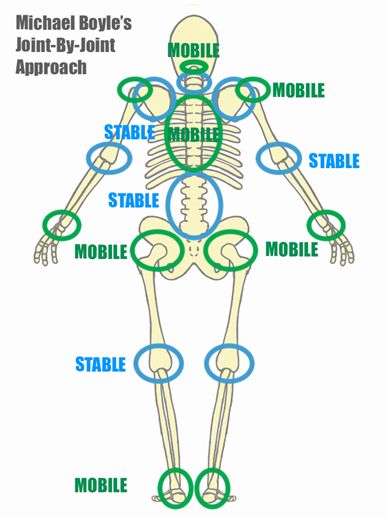
The interesting and intuitive thing about the joint-by-joint is that it alternates between the two. See below:
| Joint | Mobility vs. Stability | |
| Big toe | Mobility | |
| Mid-foot | Stability | |
| Ankle | Mobility | |
| Knee | Stability | |
| Hip | Mobility | |
| Lumbar Spine | Stability | |
| Thoracic Spine | Mobility | |
| Cervical Spine | Stability | |
| Shoulder | Mobility | |
| Elbow | Stability | |
| Wrist | Mobility | |
While this is a basic breakdown of the joint-by-joint approach, there are some exceptions to this, such as the mid-cervical spine requires stability, however, the upper two levels of the cervical spine (C1 and C2) need to be mobile. Similarly, the shoulder girdle (collarbone and shoulder blades) needs to be stable while the shoulder itself needs to be mobile.
This works great when each segment is moving as it should as each joint feeds the vulnerabilities and strengths of the other joints around it. BUT here is where the chain breaks down: for example, what if you cannot fully extend your toe? Maybe it is arthritic, maybe your plantar fascia is tight, maybe you broke it and now it is stiffer than it previously was. Because your big toe is not moving as best it could, now you are asking for your mid-foot to become more mobile, which is not the joints most effective role anatomically. Consequentially, your ankle, knee, and hip are going to adjust their roles to cover up the lack of range at the big toe. Who would have thought a big toe could make such a difference!
The human body is so great at adapting movement and finding the path of least resistance. This usually works in our favour as it is designed to conserve energy or avoid pain, however, as anyone who has experienced injury or chronic pain would know, these compensatory patterns can be detrimental to our long-term movement quality and recovery.
Understanding this principal is a great first step to being able to understand why you may be experiencing referral pain or unmasking the root of your pain. Having a movement professional perform a comprehensive assessment including gathering information about your injury history and undergoing a movement screening is the first and most crucial step in restoring those movement patterns and with time, easing the pain.